

When you walk into a pharmacy and find your prescription unavailable, or your doctor tells you a critical drug has been delayed, it’s not just bad luck. It’s the result of pricing pressure and shortages - two forces that have reshaped healthcare economics since 2020. These aren’t temporary hiccups. They’re structural shifts that are still affecting how much you pay, how long you wait, and whether you even get the treatment you need.
Why Healthcare Items Are Vanishing
In 2021, hospitals across the U.S. reported shortages of over 100 essential medications, including antibiotics, anesthetics, and insulin. The World Health Organization confirmed that more than 50 countries faced critical drug shortages during the peak of supply chain chaos. This wasn’t random. It was the result of three overlapping problems: disrupted manufacturing, labor shortages in production facilities, and sudden spikes in demand. Take antibiotics, for example. About 70% of the world’s active pharmaceutical ingredients (APIs) are made in just two countries: India and China. When lockdowns hit China in early 2022, and India restricted exports to protect its own supply, production lines stalled. By mid-2022, the U.S. saw a 40% drop in the monthly shipment of key antibiotics. Hospitals had to ration doses. Patients waited weeks for replacements. Meanwhile, demand didn’t drop. In fact, it rose. Post-pandemic, chronic illness diagnoses surged. People delayed care during lockdowns, then flooded clinics once restrictions lifted. The result? A perfect storm. Fewer inputs. More demand. Prices shot up.How Pricing Pressure Works in Health Markets
Pricing pressure isn’t just about companies raising prices. It’s about markets breaking. When supply can’t keep up, prices should rise to balance demand. But in healthcare, that doesn’t always happen - because of regulations, insurance contracts, and price caps. In the UK, the government set a cap on energy prices in 2021. It was meant to protect households. But it had a side effect: energy-intensive drug manufacturers couldn’t cover rising electricity and gas costs. Between August and December 2021, 27 small pharmaceutical suppliers went bankrupt. That didn’t just hurt their workers - it cut supply chains. A single plant shutdown can remove 15% of a drug’s global supply. In the U.S., Medicare and Medicaid set fixed reimbursement rates. If a drug’s cost jumps 30%, but the government won’t pay more, providers face a choice: absorb the loss, reduce inventory, or stop offering the drug. Many chose the last option. A 2023 study from the American Journal of Managed Care found that 18% of hospitals stopped stocking at least one essential drug because of cost pressures. This isn’t about greed. It’s about broken incentives. When prices can’t rise to reflect reality, scarcity follows. And when scarcity hits, people panic-buy. Pharmacies report spikes in early refills - sometimes 3x the normal volume - because patients fear running out. That makes shortages worse.Who Pays the Real Cost?
The most visible cost is higher prices. But the hidden costs are worse. Patients delay care. A 2022 survey by the Kaiser Family Foundation found that 34% of Americans skipped a recommended treatment because of cost or availability. That’s 1 in 3. For diabetics, skipping insulin for even a few days can mean emergency hospitalization. For cancer patients, missing a chemotherapy window can reduce survival chances by 15%. Health systems pay too. Hospitals spent an extra $12 billion in 2022 just to secure alternative suppliers or pay premium shipping fees. The Cleveland Federal Reserve estimated that supply shocks in healthcare raised core medical inflation by 0.3% in 2022 - nearly triple the effect of general goods inflation. That’s not a small number. It’s enough to push entire insurance premiums higher. Employers feel it. Companies with self-insured health plans saw claims rise 18% in 2022. Many raised employee contributions or cut coverage. Small businesses, especially, couldn’t absorb the shock. A 2023 survey by the National Federation of Independent Business showed that 41% of small employers reduced or eliminated health benefits due to rising drug and supply costs.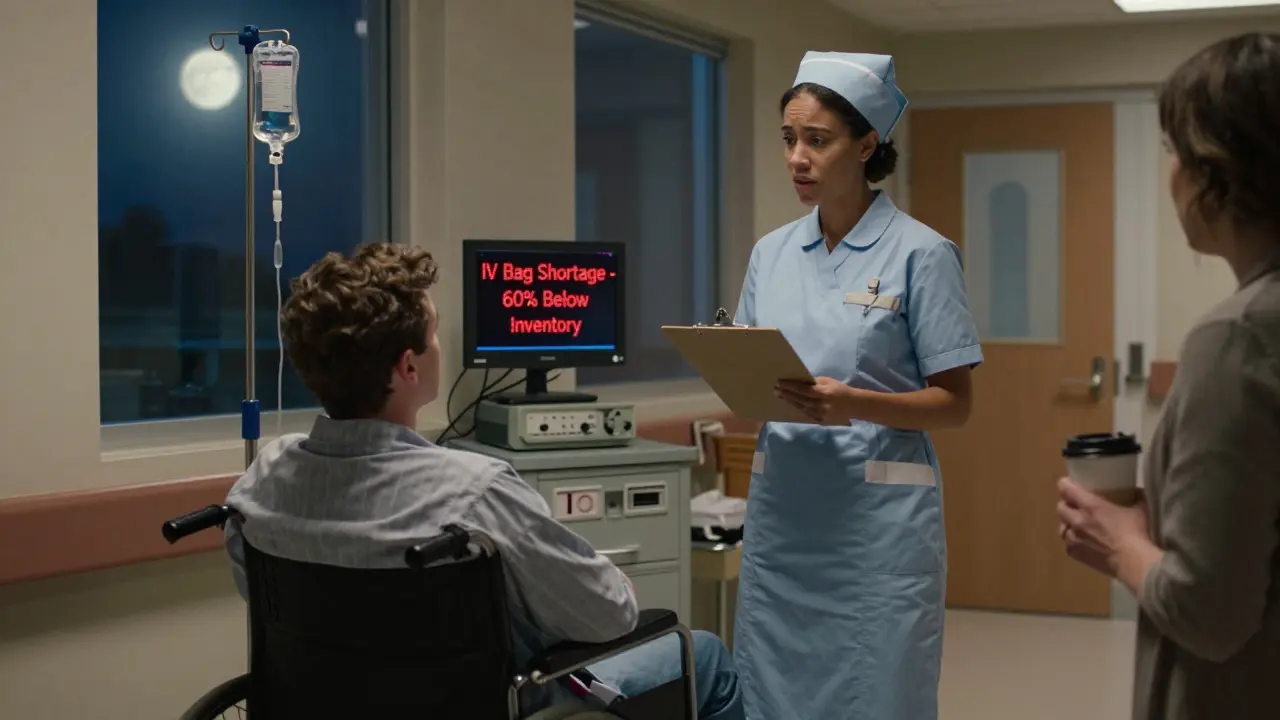
Supply Chain Shortfalls That Hit Close to Home
It’s not just pills and syringes. Think about the simple things: IV bags, catheters, glucose test strips. These are low-cost items - but they’re made in high-volume factories with thin margins. When energy prices spike, or shipping containers back up at ports, these items vanish first. In 2022, the U.S. saw a 60% increase in shortages of IV fluid bags. Why? The main manufacturer, a company in Puerto Rico, lost power during Hurricane Fiona. The backup plant in Germany was already running at 110% capacity. No one had spare capacity. No one had a plan B. The same thing happened with insulin pens. A single factory in Germany, responsible for 30% of global supply, had to shut down for 11 weeks due to labor shortages. The result? A 22% price increase in the U.S. and a 3-month wait for patients in rural areas. Even medical devices like ventilators and dialysis machines faced delays. The global supply chain pressure index for medical equipment peaked at 4.1 in December 2021 - more than 25 times its pre-pandemic level. Hospitals postponed elective surgeries. Patients waited. Some died waiting.What’s Being Done - and What’s Not Working
Governments tried to fix this. The U.S. passed the Drug Supply Chain Security Act in 2023, requiring better tracking of drug shipments. The European Union launched a €1.8 billion fund to rebuild API production on its soil. But these are long-term fixes. They won’t help today’s patients. Some companies are adapting. Pfizer and Novo Nordisk now maintain dual-sourcing for 80% of their critical inputs. That means two suppliers for every key ingredient. It costs more - but it cuts risk. Companies using this strategy saw 35% fewer disruptions in 2023. Digital tools are helping too. Hospitals using AI-powered inventory systems reduced stockouts by 28%. They can now predict shortages weeks in advance, based on global shipping data, weather patterns, and production reports. But the biggest problem remains: rigid systems. Insurance companies still pay fixed rates. Regulators still cap prices. Manufacturers still rely on single-source suppliers. Until these structures change, shortages will keep coming - and prices will keep rising.The Future Won’t Be Calmer
The San Francisco Federal Reserve says global supply chain pressure has returned to pre-pandemic levels. But that’s misleading. The baseline has shifted. Climate events, geopolitical conflicts, and labor shortages aren’t going away. The World Bank estimates that climate-related disruptions will increase medical supply delays by 15-20% annually through 2030. Nearshoring - moving production closer to home - sounds smart. But it’s expensive. Making insulin in Ohio instead of India raises production costs by 40%. That cost gets passed on. Patients will pay more. Or they’ll go without. The truth is, we’ve seen this before. In the 1970s oil crisis, gas lines formed because prices were capped. People hoarded. Gas stations ran dry. The same thing is happening with medicine. When you prevent prices from adjusting, you don’t stop inflation - you just make shortages worse.What You Can Do
You can’t fix global supply chains. But you can protect yourself. - Ask your doctor about alternatives. If your drug is on shortage, there’s often a generic or similar medication that works just as well. - Use mail-order pharmacies. They often have better inventory than local stores. - Don’t stockpile. Buying extra doses doesn’t help. It makes shortages worse for others. - Track your prescriptions. Use apps like GoodRx or your insurer’s portal to see real-time availability. - Advocate. Tell your representatives that healthcare supply chains need investment, not just price controls. This isn’t about politics. It’s about survival. Medicines aren’t commodities. They’re lifelines. And when the system breaks, the people who suffer first are the ones who need them most.Why do drug shortages happen even when demand is steady?
Drug shortages often stem from supply-side failures - not demand spikes. Most medications rely on a handful of global factories for active ingredients. If one plant shuts down due to labor strikes, power outages, or regulatory issues, supply can drop by 30-50% overnight. With no backup suppliers, even steady demand leads to shortages. For example, in 2022, a single fire at a German insulin pen factory cut global supply by 30%, triggering shortages across North America and Europe.
Can price controls prevent higher drug costs?
Price controls often make shortages worse. When prices are capped below market levels, manufacturers lose incentive to produce or invest in new supply. In the UK, energy price caps in 2021 led to 27 small pharmaceutical suppliers going bankrupt because they couldn’t cover rising production costs. The result? More drug shortages, not fewer. Markets need price signals to balance supply and demand - without them, scarcity follows.
Are generic drugs less affected by shortages?
No - generics are often more vulnerable. Because they’re sold at low margins, manufacturers rarely invest in backup production lines or diversified suppliers. In 2022, 62% of all U.S. drug shortages were for generic medications, including antibiotics, insulin, and heart medications. These drugs make up 90% of prescriptions but only 20% of spending - so they’re the first to be cut when costs rise.
How do supply chain issues affect rural healthcare?
Rural areas suffer most. They rely on fewer distributors and have less inventory buffer. When shipments are delayed, local pharmacies can’t get replacements for weeks. A 2023 study in the Journal of Rural Health found that rural patients waited 22 days longer on average for critical medications than urban patients. In some cases, patients had to drive over 100 miles to fill prescriptions - and many couldn’t.
Is nearshoring a real solution to drug shortages?
Nearshoring helps, but it’s not a quick fix. Moving drug production to the U.S. or Europe reduces shipping delays and geopolitical risk. But it increases costs by 30-40%. That means higher prices for patients and insurers. The U.S. government is investing billions to rebuild domestic API capacity, but full production won’t resume until 2027-2028. In the meantime, shortages will continue.




Brooke Exley
22 February 2026Wow. This post hit me right in the gut. I’ve been managing my mom’s diabetes for years, and last winter we went 6 weeks without her insulin pens. No joke. We had to call 12 pharmacies before one had a single vial left. It’s not about politics-it’s about survival. I’m so glad someone finally laid this out without sugarcoating.
And yeah-mail-order saved us. We switched to CVS mail and haven’t had a hiccup since. Seriously, if you’re on a chronic med, don’t wait until you’re desperate. Set it up now. Your future self will thank you.
Lisandra Lautert
24 February 202634% skipped treatment. 18% of hospitals stopped stocking essentials. 60% spike in IV bag shortages. This isn’t a crisis-it’s a systemic collapse.
Lou Suito
25 February 2026Let me get this straight-you’re blaming price caps for shortages? Please. The real issue is monopolies. Four companies make 80% of the world’s APIs. That’s not supply chain-it’s cartel behavior. And now you want us to believe that letting prices soar is the answer? No. Break up Big Pharma. Tax their excess profits. Fund domestic production. That’s real policy. Not this neoliberal hand-wringing.
Also-why is no one talking about the fact that 90% of insulin is made by three companies? Three. That’s not a market. That’s a hostage situation.
Khaya Street
26 February 2026Interesting analysis. I’m from South Africa-we’ve had these issues for decades. But here, it’s not just about pricing. It’s about logistics. No roads. No refrigeration. No reliable borders. We don’t even get the shortages you’re talking about-we get nothing. And the ‘advocate’ advice? Cute. Most of my neighbors can’t afford a phone, let alone a GoodRx app.
Maybe instead of telling people to ‘use mail-order,’ we should fix the damn infrastructure first?
Bhaskar Anand
28 February 2026India and China are the problem. We make 70% of the world’s APIs. You Americans rely on us for your lifesaving drugs. Then you call us ‘unreliable’ when we prioritize our own people during a crisis? Hypocrites. You want stability? Stop exploiting our labor, our factories, our environment. Then maybe we’ll think about your shortages.
And don’t act like nearshoring is a solution. You think making insulin in Ohio is cheaper? It’s not. It’s just more profitable for your CEOs. Meanwhile, our workers are left with nothing. Again.
Shalini Gautam
2 March 2026Bro. You’re right. India is the backbone of global pharma. But we’re not the villains. We’re the ones working 14-hour shifts in 40°C heat just to keep your insulin flowing. And now you want us to build new plants with zero investment? No. We need fair partnerships. Not lectures.
Also-why is no one mentioning the fact that Indian generics are 90% cheaper? That’s why your system even works. If you cut us off, your prices will explode. Not because we’re greedy. Because we’re the only ones still producing.
Joseph Cantu
2 March 2026They don’t want you to know this-but the real reason drugs are disappearing is because the government is secretly stockpiling them for FEMA camps. You think the VA is running out of insulin? Nah. They’ve got warehouses full. Meanwhile, grandma’s on the sidewalk waiting. That’s not a supply chain issue. That’s intentional. They want you weak. Dependent. Controlled.
And the ‘AI inventory systems’? Total scam. They’re just tracking your prescriptions so your insurer can deny you later. I’ve seen it. My cousin’s cancer med was ‘unavailable’-but the pharmacy had 12 bottles in the back. They just didn’t want to pay for it.
Don’t trust the system. It’s rigged. And they’re laughing at us.
John Smith
4 March 2026Wow. What a groundbreaking revelation. Prices can’t rise so shortages happen. Shocking. Next you’ll tell me water is wet.
Also, ‘advocate to your reps’? How adorable. You really think Congress gives a damn about your insulin? They’re too busy getting paid by Pfizer to care. You’re not fixing anything. You’re just doing performative activism while they laugh all the way to the bank.
And yes-I know you’re gonna say I’m cynical. I’m not cynical. I’m accurate.
Joanna Reyes
4 March 2026I’ve worked in hospital pharmacy for 18 years. I’ve seen this play out. The ‘perfect storm’ isn’t a metaphor-it’s a daily reality. We don’t just run out of insulin-we run out of IV tubing, catheters, even alcohol swabs. It’s not just about cost. It’s about how fragile the entire system is.
One fire. One hurricane. One labor strike. And everything collapses. We’ve had zero investment in redundancy. Zero planning. Zero foresight. And now we’re surprised people are dying because they couldn’t get a simple glucose test strip?
The AI tools help-but they’re Band-Aids. What we need is a national strategic stockpile. Not for politicians. For patients. And we need to fund it now, not in 2027.
And yes-I agree with the mail-order advice. But only because local pharmacies are being forced to operate on 24-hour inventory. It’s not their fault. It’s the system’s.
Christopher Wiedenhaupt
6 March 2026good post. i work in supply chain for a med co. we have dual sourcing now. costs more. but we dont have shutdowns like before. also-dont stockpile. it makes it worse. i’ve seen it. people buy 3 months worth. then the next person cant get anything. its not helpful. its selfish.
also-generics are the first to go. because margins are thin. no one invests in backup. so when one factory dies, 60% of the market vanishes. its insane. but its true.
Cory L
6 March 2026Real talk: we’re treating medicine like a commodity. It’s not. It’s oxygen. You don’t ration oxygen. You don’t cap its price. You don’t outsource its production to two countries and hope for the best.
We need to treat healthcare infrastructure like we treat power grids or water systems. National priority. Public investment. Redundancy. Resilience.
And yeah-nearshoring costs more. But so does burying people because they couldn’t get a shot of antibiotics.
What’s the real price?
tia novialiswati
7 March 2026Thank you for writing this 💙 I’ve been crying over my daughter’s asthma inhaler shortage for weeks. We’ve had to switch brands three times. Each time, her lungs react differently. It’s terrifying. I didn’t realize how many others were going through this. Please-keep talking. We need more voices like yours.
Also-mail-order saved us. And I stopped hoarding. My pharmacist said it helped. So I’m sharing this with my mom’s support group. 💪
Brooke Exley
8 March 2026Just saw someone say ‘don’t stockpile’-YES. This. So many people think buying extra helps. But it’s like hoarding toilet paper in 2020. It just makes it worse for the people who need it most. I wish more pharmacists would post signs: ‘Buying 3 months’ supply = someone else goes without.’